Most organizations pay shift-based clinical roles per shift or hour worked. In that model, analyzing efficiency is essentially solving a math problem. We’re asking the question, “if I have X number of physicians working Y number of Z-hour shifts, how much am I paying?”. Subsequently, we’re also inevitably asking, “if I change any of those variables can I save a few bucks?”. This is, at its core, the same question that businesses in shift-based models ask across industries. Atul Gawande compared healthcare processes to operations at The Cheesecake Factory; my favored comparison is McDonalds.
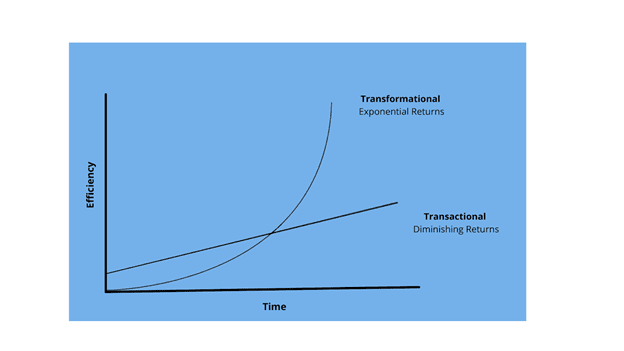
At McDonalds, staffing schedules are shift-based; employees are paid based on when they show up and when they leave. In this model, efficiency means running a restaurant with the lowest staffing costs possible to keep the griddle churning out burgers and to serve as many customers as possible in a timely fashion. It is a transactional approach to efficiency; there are only so many places to find efficiencies, and once you’ve found them, your time scrutinizing shift schedules generates diminishing returns and the savings flatten out. To identify and create real efficiencies – financial and otherwise – requires looking not just at staff schedules, but optimizing for the actual work product achieved during a single shift, with an eye towards both short- and long-term returns.
By default, we tend to think of clinical staffing efficiency from a short-term, constrained perspective (“how many RVUs were generated in this shift/month/year?”). A physician might work to hit or exceed RVU targets in the set timeframe, but those results are fleeting. There’s no momentum from that effort that propels their efficiency to greater heights over subsequent years, or that creates a ripple effect from that physician’s efficiency to their colleagues or a broader team.
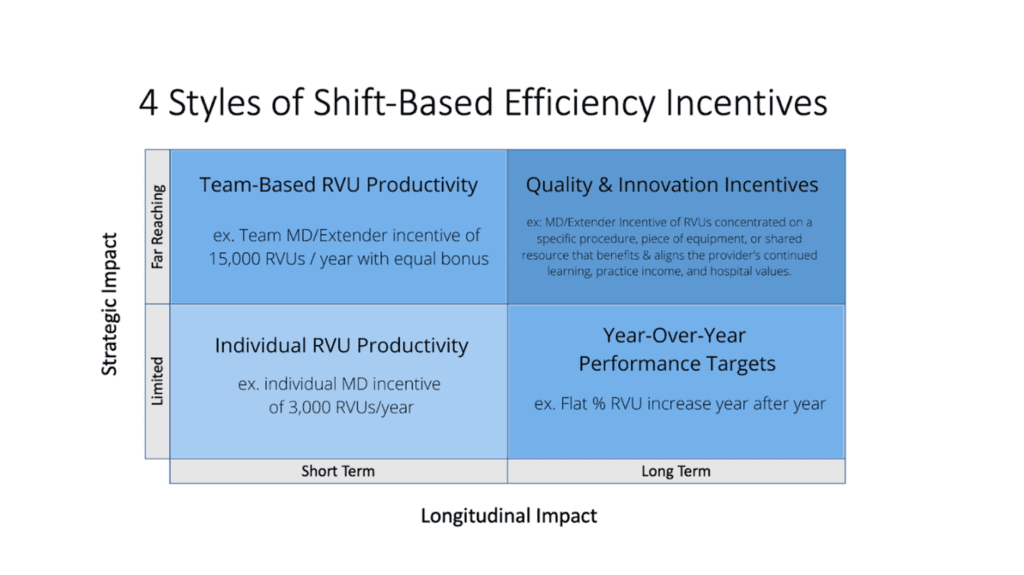
A more strategic approach shifts the focus from an exclusively production-based model to a model that allocates time and cost to longer-term efforts. This strategic approach usually generates exponential returns compared to the standard calculated efficiencies of a shift-based schedule. For example, a team of 10 clinicians generates 30,000 wRVUs annually, at $42/wRVU. Targeting a 5% productivity increase through efficiencies – a big win for most groups! – would generate an additional $63,000. On the other hand, if those 10 clinicians feel overworked or understaffed in the effort to achieve that goal and just one of them leaves as a result, that generates a cost of $500,000-$1,000,000 between the lost revenue and incurred costs to hire a replacement.
Staffing is a particularly timely example, given the staffing challenges that many provider organizations currently face, but the downstream financial impacts of shift-based staffing model decisions are far-reaching beyond clinician churn. Studies have shown that ICU patients’ length of stay, likelihood of complications, and readmissions are all affected by the length of shift that is used to staff the unit[1].
Staff wellness and injury are also correlated to shift length and schedule[2], and can be equally costly to a healthcare organization. Other studies support an annualized shift-based approach[3], which includes load-balancing shifts over the course of a year, rather than allocating a set number of shifts on a weekly or monthly basis. Additional variable staffing models optimize for the normal ebb and flow of patient volume[4], enabling more nimble staffing for these anticipated patient surges.
All of these shift-based schedule tweaks are capable of producing significant, lasting efficiencies that can be easily implemented across teams, units, and entire organizations, if only the right questions are asked when it comes time to analyze staffing models for efficiency. Although it may be counterintuitive and counterculture, creating a cushion of extra time, staffing, and other resources is where the transactional relationship with shift-based staff ends and a collaborative relationship to build better begins. These strategic, transformational approaches to the shift-based staffing model demand a forward-thinking leadership team and more thoughtful analysis, but generate outsized efficiencies.
[1] Bollschweiler E;Krings A;Fuchs KH;Pistorius G;Bein T;Otto U;Muhl E;Backes-Gellner U;Hölscher AH; “Alternative Shift Models and the Quality of Patient Care. an Empirical Study in Surgical Intensive Care Units,” Langenbeck’s archives of surgery (U.S. National Library of Medicine, 2001), https://pubmed.ncbi.nlm.nih.gov/11374042/.
[2] IOSH, “The Effects of Shift Work on Health, Summary Report,” The Effects of Shift Work on Health (IOSH), accessed February 18, 2022, https://iosh.com/media/1572/the-effects-of-shift-work-on-health-summary-report.pdf.
[3] Egbert van der Veen et al., “A Case Study of Cost-Efficient Staffing under Annualized Hours,” Researchgate (Springer Science+Business Media, 2014), https://www.researchgate.net/profile/Erwin-Hans/publication/265642369_A_case_study_of_cost-efficient_staffing_under_annualized_hours/links/02e7e53c3bd5abe6bd000000/A-case-study-of-cost-efficient-staffing-under-annualized-hours.pdf.
[4] Jenny Korth, “Variable Staffing Models at Work,” Variable staffing models at work (MGMA, August 1, 2015), https://www.mgma.com/resources/operations-management/variable-staffing-models-at-work.