In recent years, demand for medical services has increased significantly due to a growing and aging US population. To aid in managing this increased demand, many healthcare providers have expanded utilization of nurse practitioners, physician assistants, and certified registered nurse anesthetists (“CRNAS”), commonly referred to as advanced practice clinicians (“APCs”). APCs are licensed practitioners, typically with an advanced or graduate level of education, who can provide clinical care and may bill insurers for their services.
Evidence of increased APC utilization can be seen in the year-over-year changes in the number of Physicians vs. APCs billing Medicare between 2014-2019 is illustrated in the charts below[1]:
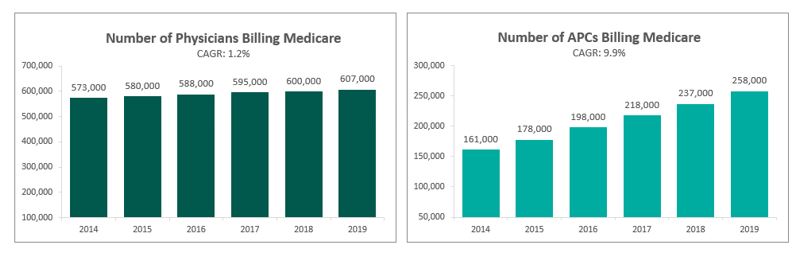
As APCs can typically perform some of the same services as physicians, but at a significantly lower cost, they can increase the economic efficiency and bottom-line profit for health systems and independent provider groups. However, as APCs do not possess all the training and credentials as their physician counterparts, physician supervision of APC services is often required to ensure the delivery of high-quality patient care. In arrangements in which physicians supervise health system or hospital-employed APCs, it is becoming more common to compensate physicians for their APC supervision services. In Gallagher’s 2020 Physician Compensation and Production Survey, over 13% of physician respondents in the specialties of family medicine and general internal medicine receive APC supervision compensation. This raises the question for health systems and independent provider groups of how to compensate physicians for APC supervision services.
While the most obvious method of compensating a physician for APC supervision would seemingly be a time-based approach, it can be difficult to confirm an accurate assessment of the number of hours a physician provides supervision or assistance to APCs. The staggered nature of supervision services (five minutes here and there throughout the day reviewing charts, fielding questions, etc.) can make it challenging to accurately log time for these services. As such, it is more common to see supervision services being compensated via other methods, as further described below.
Common APC Supervision Compensation Mechanisms
The following section addresses some common methods for compensating physicians for APC supervision services:
- Monthly or Annual Stipend – One of the most widely-used methods of compensating physicians for APC supervision services is via an annual or monthly stipend. This stipend is often calculated based on the number of APC FTEs the physician supervises, yielding a higher amount for physicians who oversee multiple APCs under the assumption it would require a more significant time commitment from the supervising physician. Similarly, if two physicians share supervision duties of one APC FTE, each physician’s stipend would be less than that of a physician who is solely responsible for supervising one APC FTE.
- Share of APC Work RVU Productivity – While compensating physicians for APC supervision services based on the supervised APC’s work RVU productivity is less commonly observed in practice, this method can incentivize and reward physicians for operating a productive practice. Under this compensation method, a physician may receive a set dollar amount per-work-RVU produced by APCs under supervision. While tying the physician’s supervision compensation to a variable measure of work product offers the physician credit for APC productivity under supervision, it is recommended that the resulting maximum annual APC supervision compensation resulting from the per-WRVU payments be capped to avoid overpayment.
- Blended Stipend plus Work RVU Productivity – A blend of the two methods described above has also been observed in the market to compensate physicians for base time spent providing general supervision while still offering incentive to operate a productive practice.
- Profit Allocation – An income-based approach, this method compensates physicians for APC supervision services based on a portion of the profits generated from the APC’s professional services, after subtracting all relevant expenses related to the APC’s services from the professional collections generated by the supervised APC.
Potential Compliance Pitfalls
The below section covers some potential compliance pitfalls related to APC supervision compensation:
- Double-Counting – There are several scenarios in which compensating physicians for APC supervision could be inappropriate or viewed as duplicative of other compensation.
- PSAs in Which Group Is Paid for APC WRVUs: In a professional services agreement in which the provider group is already compensated at a fair market value rate for work RVUs produced by APCs, paying a separate compensation amount to the Group for APC supervision could be viewed as duplicative, as the provider group is already being compensated for the APC productivity via the WRVU rate.
- Time-Based Clinical Compensation: Similarly, if a physician is compensated for clinical services via an annual salary based on his/her full-time equivalent (“FTE”) status, paying the physician incremental APC supervision compensation could be viewed as paying twice for the same hour of service unless the supervision hours are above and beyond the physician’s clinical FTE status.
- Billing and Collection Rights: In arrangements in which a physician or physician group is able to bill and collect for APC clinical services, paying incremental APC supervision compensation could be viewed as duplicative, as the group/physician would already be receiving compensation (and potentially, profit) related to the productivity of the APCs.
- Overlooking Indirect Expenses – For income-based methodologies of APC supervision compensation, it is important for all expenses related to the APC’s clinical services to be deducted before calculating physician compensation for APC supervision. If all necessary overhead expenses are not reflected in the expenses of the APC clinical services for calculation purposes, this could lead to overpayment to the supervising physician.
- Stacking / Valuation Principles – As APC supervision compensation becomes more and more commonplace in healthcare settings, especially in primary care specialties, valuation and physician compensation professionals must be aware that total cash compensation figures reported in surveys relied upon for assessment of physician compensation may already include some amount of APC supervision compensation embedded in the survey data.
As utilization of APCs continues to increase in the healthcare industry, determining if/how to compensation physicians for APC supervision services will continue to be a topic of discussion for health systems and independent provider groups. APCs offer significant value to health systems and independent providers by allowing physicians to allocate a higher portion of their time to more specialized services. However, before paying physicians for APC supervision services, health systems should ensure that the supervision compensation arrangements are commercially reasonable and do not result in compensation that exceeds fair market value.
Matthew McKenzie, CVA, Director, VMG Health and Thomas Torcellini, Manager, VMG Health
[1] Information sourced from the March 2021 Report to the Congress: Medicare Payment Policy.